Some long-term or repeated exposure to medications that affect dopamine pathways can lead to persistent involuntary movements. These movement changes typically involve repetitive, choreiform or rhythmic motions of the face, mouth, or limbs and may appear after weeks to years of treatment. The underlying concept centers on how sustained pharmacologic blockade of dopamine receptors in motor-related brain circuits can alter receptor sensitivity and motor control, which in turn may produce observable movement differences in some people.
Medications that interfere with dopamine signaling are most commonly discussed in connection with these delayed movement changes. The likelihood of developing such movement patterns can vary by drug class, dose, duration of exposure, and individual biological factors. Clinicians and researchers often distinguish between short-term drug-induced movement side effects and those that persist or emerge after prolonged use; the latter tend to be more complex to assess and manage and may follow different time courses.
Comparative patterns across these examples show differences in pharmacology and apparent risk profiles. Typical antipsychotics tend to exhibit stronger dopamine D2 receptor antagonism, which has been associated with a greater frequency of delayed movement sequelae in some clinical series. Atypical antipsychotics often have mixed receptor activity that may lower but not eliminate the potential for movement changes. Antiemetics that block dopamine receptors can produce similar motor effects when exposure is prolonged or cumulative. These are general patterns and individual outcomes can vary.
Risk factors that may influence whether movement changes develop include cumulative dose, duration of exposure, older age, and coexisting neurological or metabolic conditions. Polypharmacy—concurrent use of multiple drugs that affect motor pathways—can increase the complexity of risk assessment. Genetic and individual vulnerability factors may also play a role, and these are active areas of clinical study. Estimates of prevalence vary across studies and settings, and reported rates typically depend on the population and exposure timeline assessed.
Symptom presentation commonly involves involuntary oral-facial movements such as lip-smacking, tongue protrusion, or jaw movements, and may also include limb or truncal movements. Onset can be delayed, sometimes appearing after medication reduction or cessation. In practice, clinicians often use standardized examinations to document and track movement patterns over time to differentiate transient drug-induced effects from persistent or progressive movement disorders. Duration and progression of symptoms can be variable.
Monitoring practices may include baseline documentation of motor function before starting an agent with dopamine-blocking activity and periodic re-evaluation during therapy. Clinical rating tools and structured observation may help detect subtle early signs. Communication among prescribing clinicians, primary care providers, and patients or caregivers about possible movement changes supports timely assessment. Reporting observed medication-associated movement changes to regulatory or pharmacovigilance systems is an informational step clinicians may consider to contribute to safety data.
In summary, medications that alter dopamine signaling can be followed by persistent or delayed involuntary movement changes in some people; risk is influenced by drug class, exposure patterns, and individual factors. Understanding typical symptom patterns, monitoring approaches, and comparative pharmacologic features helps frame clinical assessment without implying uniform outcomes. The next sections examine practical components and considerations in more detail.
Within the broad category of dopamine-modulating drugs, distinct classes exhibit different pharmacodynamic profiles that can influence the likelihood of delayed movement changes. First-generation antipsychotics typically produce strong D2 receptor blockade and have historically been observed in clinical series to have higher incidence of persistent movement effects after prolonged exposure. Second-generation antipsychotics generally have more diverse receptor activity and may present a different risk profile, though some agents within this group remain associated with delayed movements in clinical reports.
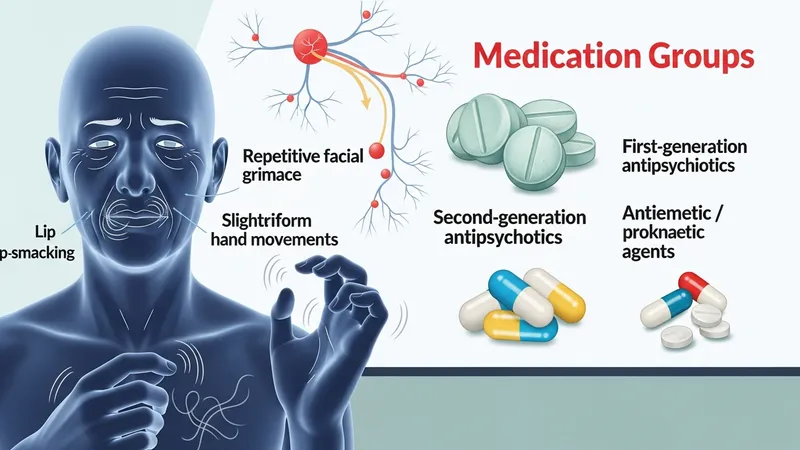
Antiemetic agents that antagonize dopamine receptors, such as certain prokinetic drugs, may also be implicated when exposure is prolonged or at higher doses. These medications are often used for gastrointestinal indications and can produce similar motor effects because they act on overlapping receptor targets in motor pathways. The risk associated with these agents is typically discussed in relation to duration and cumulative dose rather than single short-term exposures.
Comparisons across classes should be interpreted cautiously: observational studies, randomized trials, and pharmacovigilance reports may yield different estimates depending on population, follow-up length, and diagnostic criteria. Meta-analytic summaries often emphasize heterogeneity across studies. Clinicians and researchers typically evaluate both absolute exposure and relative pharmacologic potency when considering potential contribution to delayed movement changes.
Decision frameworks that examine class-specific properties often consider receptor binding affinity, half-life, and co-receptor interactions as mechanistic contributors. While these pharmacologic features may help explain observed differences in clinical patterns, they do not predict individual outcomes with certainty. Continued surveillance and careful documentation across drug classes remain central to understanding long-term motor safety.
Duration of treatment and cumulative dose are commonly reported correlates of increased likelihood for persistent movement changes; longer exposure periods typically correspond with higher observed incidence in many clinical series. Advanced age is another factor that may increase vulnerability, and some reports indicate females may be more frequently affected, though findings vary. Preexisting movement disorders, cognitive impairment, or metabolic conditions can complicate both risk estimation and clinical detection of new or worsening involuntary movements.
Symptom patterns often begin with subtle oral-facial movements and may later involve the extremities or trunk. The onset can be delayed, sometimes occurring after months or years of exposure or after drug dose reduction or withdrawal. Movement amplitude and frequency can fluctuate, and symptoms may interfere with eating, speech, or daily activities in some individuals. Patterns can be heterogeneous across cases, and standardized assessments are used to characterize severity and distribution.
Polypharmacy and drug interactions that increase exposure to dopamine-blocking effects can be a contributory consideration. Clinicians frequently evaluate concomitant prescriptions that may have additive motor effects, including both psychiatric and non-psychiatric medications. Metabolic or neurodegenerative comorbidities may alter susceptibility, and individualized assessment is often necessary to contextualize observed movement changes.
Because onset and course can be variable, longitudinal documentation is important; repeated assessments help distinguish transient, reversible drug-related effects from persistent movement patterns. Symptom evolution over weeks to months is commonly reported in observational studies, and longer-term follow-up may be needed to understand stability or progression in individual cases.
Structured clinical tools are available to aid detection and monitoring of involuntary movements; for example, clinician-rated scales are used in research and practice to quantify severity and document change over time. Baseline motor examinations before initiating a dopamine-modulating medication provide a reference for later comparison. Periodic reassessment at clinically appropriate intervals may detect early signs that otherwise could be missed during routine visits.

Patient and caregiver observations are valuable components of monitoring because involuntary movements may fluctuate and may be more noticeable in daily life than during a brief clinical exam. Encouraging accurate, objective descriptions of onset, frequency, and circumstances of observed movements helps clinicians interpret clinical findings. Video documentation, when acceptable to the patient, can supplement clinical notes for longitudinal comparison without implying any specific management steps.
Pharmacovigilance reporting systems collect information about suspected medication-associated adverse events; submitting detailed reports contributes to the broader evidence base. Documentation typically includes drug names, dosages, duration of exposure, temporal relationship to symptom onset, and relevant medical history. Such reporting aids regulators and researchers in identifying patterns and potential safety signals across populations.
Educational resources for clinicians and patients often emphasize recognition and documentation rather than prescriptive actions. Monitoring strategies generally prioritize early identification and careful clinical evaluation, recognizing that individual circumstances determine subsequent clinical decisions. Clear recordkeeping supports both individual care and aggregated safety surveillance efforts.
When movement changes are identified, clinical considerations typically involve a careful review of the medication history, assessment of potential contributing factors, and discussion among treating clinicians. Decisions about altering therapy are individualized and often weigh the therapeutic benefits of the medication against potential motor risks. Shared decision-making and clear documentation of risks discussed may support clinical care without implying a single correct action for all situations.

Regulatory agencies and professional societies periodically issue safety communications or guidance that contextualize evolving evidence on medication-associated movement effects. Such guidance can include information about known risks, recommended monitoring intervals, and reporting pathways. Clinicians often consult current regulatory summaries and peer-reviewed literature to inform practice, recognizing that evidence may change over time as new studies emerge.
Communication with patients and caregivers focuses on describing observable signs to watch for, documenting baseline function, and setting expectations for follow-up evaluation. Informational conversations are typically framed around monitoring and assessment rather than promises about outcomes. Clear explanation of the uncertainties and potential timelines for onset or change helps set realistic expectations for detection and ongoing care.
Ongoing research continues to refine understanding of mechanisms, risk stratification, and long-term outcomes. Clinicians and researchers typically approach new findings cautiously, integrating updated evidence into practice guidelines and monitoring strategies as the evidence base grows. Readers interested in more detailed clinical guidance are advised to consult authoritative clinical resources and recent literature for context-specific recommendations.